Below are the compilation of all the eponymous signs in ENT from all over the net.Read & enjoy..
AQUINO'S SIGN is the blanching of the tympanic mass with gentle pressure on the carotid artery.Seen in Glomus tumors .
BATTLE SIGN- Bruising behind ear at mastoid region, due to petrous temporal bone fracture (middle fossa #)

BEZOLD'S SIGN / SYMPTOM
Inflammatory edema at the tip of the mastoid process in
mastoiditis
BOCCA’S SIGN - Absence of post cricoid crackle(Muir’s crackle) in Ca post cricoid
BROWNE'S SIGN
Refers to the blanching noted when applying positive pressure{with Siege's speculum} to the tympanic membrane of a patient with Glomus tumor.
BRYCE SIGN - If combined laryngocele & external laryngocele is presenting as a neck mass, compression will cause a hissing sound as the air escapes from it into the larynx. This test is fraught with danger in cases of combined laryngoceles because air from the external component may get forced into the internal component causing acute airway obstruction.
DELTA SIGN
Lateral sinus thrombosis on CT or MRI with contrast shows an empty triangle appearance of the thrombosed sinus surrounded by contrast enhanced dura{since contrast may flow around the clot to outline the periphery of the sinus}. It is also called as empty triangle sign. 
DODD’S SIGN/CRESCENT SIGN- X-ray finding-Crescent of air between the mass and posterior pharyngeal wall. positive in AC ployp Negative in Angiofibroma
FURSTENBERG'S SIGN-Positive in Encephaloceles.Owing to the intracranial connection, there is pulsation and expansion of the mass with crying, straining, or compression of the jugular vein (Furstenberg test).This is used to differentiate Nasal Encephaloceles from other congenital midline nasal masses like Nasal Gliomas.
GRIESINGER'S SIGN-Erythema and oedema posterior to the mastoid process resulting from septic thrombosis of the mastoid emissary vein. seen in lateral sinus thrombosis
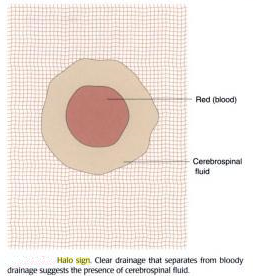
HALO SIGN/ HANDKERCHIEF SIGN - A finding in CSF rhinorrhea when CSF is mixed with Blood.
- In patients with head trauma, a mixture of blood and CSF may make the diagnosis difficult.
- CSF separates from blood when it is placed on filter paper, and it produces a clinically detectable sign: the ring sign, double-ring sign, or halo sign.
- CSF will separate from blood when the mixture is placed on filter paper resulting in a central area of blood with an outer ring or halo.
- Blood alone does not produce a ring.
- The best ring is obtained with a 50: 50 mix of blood and CSF.
- More importantly, they found that the presence of a ring was not exclusive for CSF.
- Blood mixed with tap water, saline, and rhinorrhea fluid also produced a ring.
- The halo sign does occur, but clearly does not clinch the diagnosis.
HITSELBERGER’S SIGN - In Acoustic neuroma- loss of sensation in the postero-superior part of external auditory meatus supplied by Arnold’s nerve( branch of Vagus nerve to ear )
HOLMAN MILLER SIGN, ANTRAL SIGN-
The anterior bowing of the posterior wall of the antrum seen on lateral skull film .Pathognomic for juvenile nasopharyngeal angiofibroma.
HONDOUSA SIGN–X-ray finding in Angiofibroma.
indicating infratemporal fossa involvement characterised by widening of gap between ramus of mandible and maxillary body.
HENNEBERT'S SIGN
It is a false positive fistula test when there is no evidence of middle ear disease causing fistula of horizontal semicircular canal. It is seen in 25% cases of meniere's disease or congenital syphilis.In 25% cases of Meneire’s ,fibrous bands form connecting utricular macule to stapes footplate. In syphilis due to hypermobile stapes footplate.[Hennebert sign- pressure induced nystagmus, Hennebert symptom- pressure induced dizziness]
IRWIN MOORE’S SIGN——– positive squeeze test in chronic tonsillitis.
LAUGIER'S SIGN-Blood behind the eardrum suggests basilar skull fracture.
LEUDET'S SIGN-Inflammation of the eustachian tube can produce a bright clicking sound heard by the examiner through the otoscope while the patient experiences it as tinnitus.caused by reflex spasm of the tensor palati muscle.
LIGHT HOUSE SIGN—A small pin hole perforation with a pulsatile ear discharge is seen in Acute suppurative otitis media.
LYRE’S SIGN - splaying of carotid vessels( at junction of External & internal carotid artery) in carotid body tumor.
MILIAN’S EAR SIGN- Erysipelas can spread to pinna(cuticular affection), where as cellulitis cannot.
Cellulitis and erysipelas manifest as areas of skin erythema, edema and warmth in the absence of underlying suppurative foci.
They differ in that erysipelas involves the upper dermis and superficial lymphatics, whereas cellulitis involves the deeper dermis and subcutaneous fat.
As a result, erysipelas has more distinctive anatomic features than cellulitis; erysipelas lesions are raised above the level of surrounding skin, and there is a clear line of demarcation between involved and uninvolved tissue.
Classic descriptions of erysipelas note "butterfly" involvement of the face.
Involvement of the ear (Milian's ear sign) is a distinguishing feature for erysipelas since this region does not contain deeper dermis tissue.

OMEGA SIGN -INFANTILE OMEGA SHAPED EPIGLOTTIS SEEN IN LARINGOMALACIA.
Paul Dudley White's winking ear lobe sign-Movement of the ear lobe coincident with the pulse suggests tricuspid insufficiency.
PHELP’S SIGN - loss of crest of bone (as seen in CT-scan) between carotid canal and jugular canal in glomus jugulare.
RAT TAIL SIGN /“Bird-beak” sign-Sign in barium swallow of achalasia. The oesophagus is dilated, and contrast material passes slowly into the stomach as the sphincter opens intermittently. The distal oesophagus has a narrow segment and the image resembles a bird's beak.
This is in contrast to the rat's tail appearance of carcinoma of oesophagus.Barium swallow shows characteristic rat tail appearance with irregular mucosa margins in carcinoma esophagus.
RISING SUN SIGN
There is red vascular hue seen behind the intact tympanic membrane. it is seen in glomus tumour, high jugular bulb and aberant carotid artery in the floor of middle ear.
RACCOON SIGN-Indicate subgaleal hemorrhage,and not necessarly base of skull .
SCHWARTZ SIGN
It is also called flamingo flush sign. it is seen because of increased vascularity in submucous layer of promontory in active phase of otosclerosis(otospongiosis).
STEEPLE SIGN- X-ray finding in Acute laryngotracheobronchitis (CROUP).The steeple sign is produced by the presence of edema in the trachea, which results in elevation of the tracheal mucosa and loss of the normal shouldering (lateral convexities) of the air column. 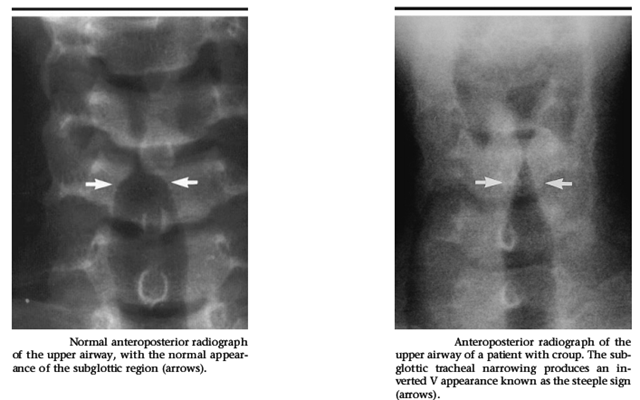
STANKIEWICK’S SIGN - indicate orbital injury during FESS. fat protrude in to nasal cavity on compression of eye ball from outside .
TEAR DROP SIGN
Seen in Orbital floor fracture. It is defined as tear drop shaped opacification seen hanging from the roof of the maxillary sinus on water's view. The floor of the orbit is the most common portion of the orbit to sustain fracture. A classic radiographic finding in blow-out fractures is the presence of a polypoid mass (the tear-drop) protruding from the floor of the orbit into the maxillary antrum The tear-drop represents the herniated orbital contents, periorbital fat and inferior rectus muscle. THUMB SIGN
It is a thumb like impression (due to enlarged epiglottis) seen on X-ray lateral view neck in patients with acute epiglottitis.Direct visualization of the epiglottis by laryngoscope, if attempted, reveals a beefy red, edematous epiglottis.
TRAGUS SIGN
In acute otitis externa there is marked tenderness when tragus is pressed against the pinna.
TEA POT SIGN is seen in CSF rhinorrhoea.This could be related to the relationship of the sphenoid ostium to the sinus floor. The sphenoid ostium lies at an appreciable distance anterosupe-rior from the sinus floor. An increase in the CSF rhinorrhea therefore occurs in a case of sphenoid sinus leak when the patient bends forward as an increasing amount of CSF gains access to the ostium "teapot" sign.
uvula pointing sign - uvula points to side of palatal palsy
Uvula pointing sign- seen in rhinoscleroma .when scleroma involve nasopharynx ,uvula point towards roof of nasopharynx.
WOODS SIGN—– palpable jugulodigastric lymphnodes.














 Alcohol intake is strictly prohibited when we take these drugs!Let us know what these drugs are.
Alcohol intake is strictly prohibited when we take these drugs!Let us know what these drugs are.
 Disulfiram irreversibly inhibits the oxidation of acetaldehyde by competing with the cofactor nicotinamide adenine dinucleotide (NAD) for binding sites on ALDH . Ultimately, disulfiram reduces the rate of oxidation of acetaldehyde, causing a 5- to 10-fold increase in the concentration of acetaldehyde. An increased serum acetaldehyde concentration is thought to be responsible for the unpleasant side effects associated with the disulfiram-ethanol reaction.source:
Disulfiram irreversibly inhibits the oxidation of acetaldehyde by competing with the cofactor nicotinamide adenine dinucleotide (NAD) for binding sites on ALDH . Ultimately, disulfiram reduces the rate of oxidation of acetaldehyde, causing a 5- to 10-fold increase in the concentration of acetaldehyde. An increased serum acetaldehyde concentration is thought to be responsible for the unpleasant side effects associated with the disulfiram-ethanol reaction.source:












 Check this
Check this 